
© Ennis Physiotherapy Clinic, 3A Barrack Close, Barrack Street, Ennis, Co. Clare V95 X437 Tel: (065) 6840757
Spinal Problems Neck + Back Pain Disc Injury Whiplash Posture
Lower Limb Injuries Walking + Running Ligament Injury Snowsports Injury Home Exs Prog
Upper Limb Injuries Ligament Sprains Tendon+Muscle Golf + Bike Set Up Useful Links



065 6840757

Mon - Fri 9.30am - 8.30pm


3a Barrack Close, Barrack St., Ennis, Co. Clare V95 X437
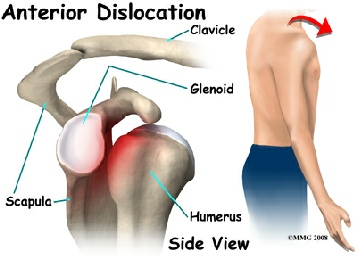
Shoulder dislocation is a common traumatic injury which can occur during sporting activity or as a result of a fall. A dislocated shoulder occurs when the humerus separates from the scapula at the glenohumeral joint. The shoulder joint has great mobility and therefore little stability and is susceptible to dislocation. A sublimation is a partial dislocation of the shoulder.
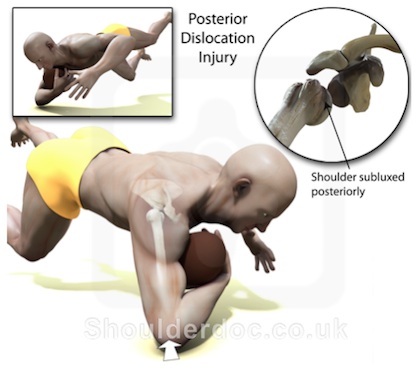
There are different types of dislocation dependent on the direction the head of the
humerus is dislocated. Over 95% of shoulder dislocation cases are forward.
Forward dislocations are usually caused by a direct blow to or fall back or to the side
on an outstretched arm. Backward dislocations are occasionally due to seizure or by
strength imbalance of the rotator cuff muscles. Patients typically present holding their
arm internally rotated and adducted, and exhibiting flattening of the anterior shoulder
and a prominent coracoid process. Downward dislocation is the most unlikely (<1%).
Signs and symptoms
- Significant pain
- Inability to move the arm from its current position
- Numbness of the arm
- Visibly displaced shoulder / flattened appearance around the shoulder. .
Shoulder Dislocation Shoulder Tendonitis
Tennis + Golfers Elbow Fractured Wrist
Fractured Finger Fractured Knuckle
‘Tennis elbow’ is a generic term used to describe an overuse injury of the tendons at the outside of the elbow, also known as lateral epicondylitis or tendonitis. ‘Golfers elbow’ is a similar condition affecting the tendons on the inside of the elbow and is also called medial epicondylitis or tendonitis.
In fact it is not necessarily associated with playing tennis or golf but more with excessive use of the forearm muscles attached to the bone at the elbow. It occurs with either excessively repetitive activity, with use of excessive gripping force with the hand or working with the hand in an awkward / poor ergonomic position.
Epicondylitis or tendonitis around the elbow responds well to treatment by
physiotherapists. Treatment may include avoiding the provoking activity for
a short period, soft tissue massage, exercises for stretching and strengthening
of the affected muscles and other tissues, adjusting work and playing
postures, adjusting sports equipment. Symptoms associated with the
inflammation of the tissues such as pain will respond well to electrotherapy
modalities and medications prescribed by a GP. A support brace can be
worn over the tendons at the upper end of the forearm muscles in order to
relieve some of the strain and to allow the injured area to ‘rest’.
For a detailed assessment and advice or treatment as necessary contact us at
Ennis Physiotherapy Clinic.


Fracture of the knuckle occurs usually as a result of direct blows or trauma to the rounded lower end of the metatarsal bone which forms what we refer to as the knuckle of the hand.
 One of the knuckles is usually slightly prominent when the fingers are closed and if the closed hand is struck hard against something solid (striking with a closed fist) there is a possibility the bone will break just behind the rounded end area.
One of the knuckles is usually slightly prominent when the fingers are closed and if the closed hand is struck hard against something solid (striking with a closed fist) there is a possibility the bone will break just behind the rounded end area.
Similarly if the open hand is struck hard by another solid object (like a ball or a hurley) it can cause a fracture of the underlying bone.
There is likely a typical appearance of bruising and swelling in the hand and fingers associated with pain and reduced or minimal active movement. Depending on the movement of the bony fragment the knuckle may become more prominent or may seem to disappear as it drops below the level of the adjacent ones.
Physiotherapy can help to restore normal
movement to the joints of the affected
fingers and dexterity in the hand in general.
For treatment and advice or an assessment
contact us directly at Ennis Physiotherapy Clinic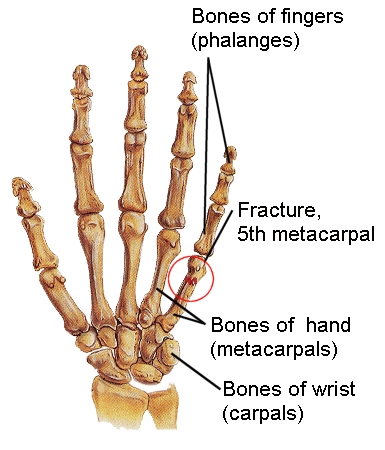
A broken wrist normally occurs after a fall onto an outstretched hand. The break occurs in the lower end of the bone(s) of the forearm. The bone fragment may tilt forward (also known as a Smith’s fracture) or backwards which is the more usual one.

There is usually severe pain and minimal active movement is possible. The area can become bruised and swollen within a short period and this can extend into the hand and fingers.
Immediate treatment is with immobilisation within a cast for a number of weeks after manipulation back into a corrected position. This followed by active use and gradual return to normal function. Where there is difficulty with returning to full range of movement or in restoring normal strength and dexterity a patient may be referred for assessment and treatment by chartered physiotherapists.
At Ennis Physiotherapy Clinic we can provide detailed assessment and personalised treatment directed at restoring the maximum amount of normal movement at the joints of the wrist and hand, at reducing any swelling present, at improving pain and functional us.
This will facilitate a return to activities of daily living as soon as possible. This can include work, sport, living or simple leisure activities

Shoulder Tendonitis / Impingement
 The shoulder joint has a very large range of movement which occurs in many directions (is multi-planar). Joints that are highly mobile, like the shoulder, tend to be more unstable. In order to achieve a high level of mobility, the shoulder depends more on dynamic stability provided by the rotator cuff muscles around the joint than on the static stability provided by the capsule and ligaments. Other factors which determine normal shoulder function is the position + movement of the shoulder blade (scapula), expansion of the AC joint downwards towards the tendons and the shape / orientation of the acromion (bony point of the shoulder).
The shoulder joint has a very large range of movement which occurs in many directions (is multi-planar). Joints that are highly mobile, like the shoulder, tend to be more unstable. In order to achieve a high level of mobility, the shoulder depends more on dynamic stability provided by the rotator cuff muscles around the joint than on the static stability provided by the capsule and ligaments. Other factors which determine normal shoulder function is the position + movement of the shoulder blade (scapula), expansion of the AC joint downwards towards the tendons and the shape / orientation of the acromion (bony point of the shoulder).
These affect the risk of developing tendonitis or impingement at the shoulder.
Tendonitis of the rotator cuff tendons of the shoulder is a common cause of shoulder pain. It is frequently due to overuse (repetitive) or over exertion in the younger person and can occur as a secondary issue to poor posture in older people with slouched postures. Repeated use of the arm, moving at or above shoulder level and especially when rotating can provoke inflammation of the tendons. A fall onto the hand or elbow or a sudden drag on the shoulder / arm can also provoke acute symptoms.
 Impingement or pinching of the tendon can occur at the shoulder between the humerus (upper arm bone) and the acromion when the upper arm is used repeatedly and vigorously at or above shoulder level. The usual movements that cause impingement are a combination of forward flexion to 900 (or more) and inward rotation of the arm. Swimmers, throwers, racquet players and weight lifters are all at risk. In the older person there are changes within the bone of the acromion, the ligaments around the shoulder and the position of the scapula which increase the risk of impingement. With repeated movement the tendons become inflamed and swell. If this becomes chronic it leads to scarring and weakens the tendon which can then tear either partially or fully.
Impingement or pinching of the tendon can occur at the shoulder between the humerus (upper arm bone) and the acromion when the upper arm is used repeatedly and vigorously at or above shoulder level. The usual movements that cause impingement are a combination of forward flexion to 900 (or more) and inward rotation of the arm. Swimmers, throwers, racquet players and weight lifters are all at risk. In the older person there are changes within the bone of the acromion, the ligaments around the shoulder and the position of the scapula which increase the risk of impingement. With repeated movement the tendons become inflamed and swell. If this becomes chronic it leads to scarring and weakens the tendon which can then tear either partially or fully.
This condition, if allowed to become chronic, may lead to significant limitation of movement and pain. It responds slowly but well to conservative forms of treatment including exercise and joint mobilisation. Increased strength and good flexibility of the muscles around the shoulder, in addition to postural retraining, all help to maintain improvement in the longer term.
For further information and an assessment please contact us at the clinic.
The following video gives an indication of some of the possible exercises that may be suitable for someone with shoulder + rotator cuff problems. An alternative video which has some more basic exercises and an explanation is at this link. These links are indicative + for information only and specific advice should be sought from your physiotherapist.
Treatments
- Prompt medical treatment should be sought for any dislocation injury. Emergency treatment will return the shoulder to its normal position by manipulation. An x-ray will confirm the joint has been reduced back into the glenoid cavity.
- The arm is likely to be rested in a sling for several days until pain subsides.and then mobilized as soon as the pain allows.
- Rotator cuff and deltoid strengthening is the focus of conservative treatment for an unstable shoulder. Trauma associated with dislocation often disturbs the normal activity of muscles supporting and moving the shoulder blade.
- First-time traumatic dislocation have a high rate of labral injury Surgery may be required following repeated dislocation.
Return to full function and early return to sport or work can be facilitated following treatment and advice from Ennis Physiotherapy Clinic.
There is usually a slow gradual onset of symptoms. Symptoms are made worse by extension of the wrist, by gripping with the hand and possibly with turning the forearm (pronation and supination). The main symptom is of pain and tenderness around the bony point on the outside (tennis) or inside (golf) of the elbow. There may be stiffness after rest periods and some creaking. Occasionally there may be signs of nerve irritation as the nerves supplying the forearm and hand pass through the affected tissues. Poor upper limb posture and imbalance in muscle work are common findings and neck and shoulder problems are also a common feature